
ACCELERATING LIFE SAVING ALTERNATIVE THERAPIES:
PATIENT INFORMATION RESOURCE
(ALSAT PIR)
PROPOSAL
Michael Gollin
mgollin@gmail.com
September 2013 Draft
This is an updated proposal benefiting from extensive input from various stakeholders including MDA, Patients Like Me, ALS Untangled, and the ALS clinics at Massachusetts General Hospital and Johns Hopkins.
Summary
There is currently no resource that provides ALS patients and caregivers with readily understood information about complementary and alternative therapy options available to them, in a format that supports informed decision-making about what therapies they should pursue. The Accelerating Life Saving Alternative Therapy Patient Information Resource (ALS AT PIR) would fill this gap with a patient-centered website that lists various supplements, medicines, diets, and practices, along with specific dosing regimens, linked to available evidence about potential benefits, harms, and costs. Patients may review the site and obtain a set of alternative therapies to discuss with their physicians. The PIR site fills the gap in patient information about existing alternative therapies by intermediating between patient self-reporting (as pioneered by Patients Like Me) and evidence-based recommendations by clinicians and researchers (building on the model of ALS Untangled). The ALSAT PIR proposal has attracted strong interest from leaders in ALS therapy, research, and patient advocacy.
Scope of the Problem:
After I was diagnosed with ALS, even with my training as a biologist and life science patent attorney, and with medical care at a leading ALS clinic, it still took me almost a year and extensive networking before I found what I consider to be a reasonable therapeutic regimen. There are about 500,000 ALS patients worldwide, with about 100,000 new cases annually. In the US, there are about 30,000 ALS patients with 5,000 new diagnoses annually. ALS patients have no adequate clinically proven therapies and it is extremely difficult for them to find adequate information about available alternative therapies that they can pursue to improve their health, function, and quality of life. This project originated in the realization that the world would benefit from a readily accessible summary/digest of current medical thinking and patient practice around ALS.
How it works:
The ALSAT PIR provides a patient information resource, positioned at the apex of an informational triangle, with patient input through a discussion group on one leg, and doctor/scientist input on the other leg. The PIR is intended to stimulate productive patient-doctor dialogue, not to be a substitute for good medical care.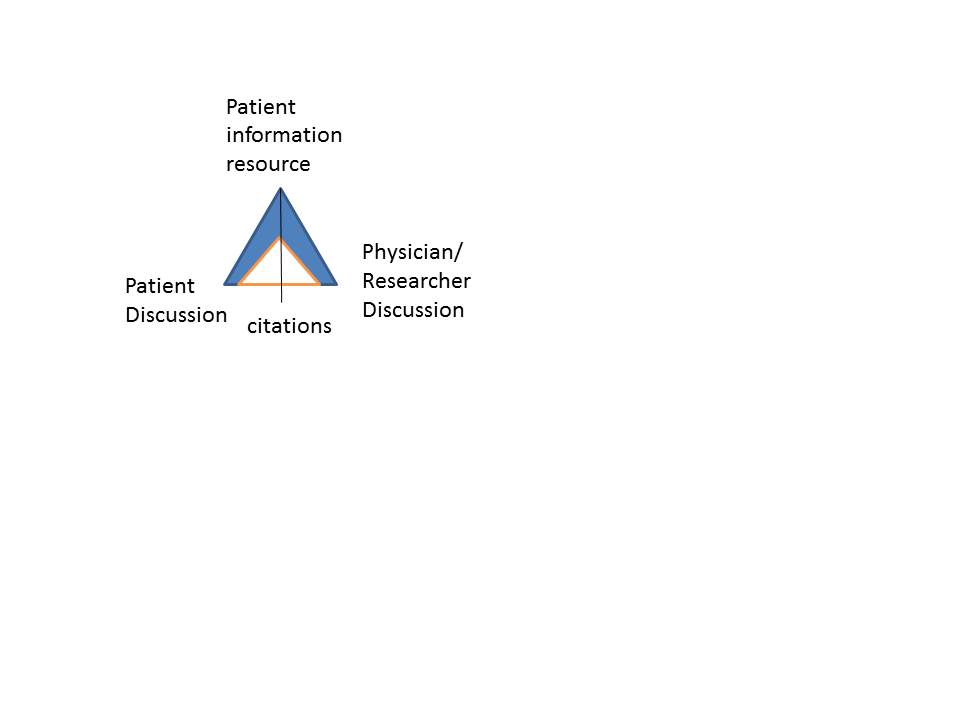
On one side is information about what patients are doing (for example, extracted from Patients Like Me). On the other side is learned commentary by clinicians and researchers (for example, a consortium like ALS Untangled). And between, at the hinge, is the Patient Information Resource, a menu of concrete options – dosing regimens – for patients to consider with their doctors (such as the regimen I was eventually able to compile). It would also include a list of therapies to avoid that are contra-indicated due to evidence of ineffectiveness, toxicity, or extreme cost. This approach has features and benefits not present in existing resources.
For example, the draft PIR in Appendix 1 lists dietary supplements recommended by ALS clinic doctors, along with daily dosage (mg or IU) and dosage regimen (1x/d or 2x/d) plus any recommended blood tests or other monitoring or diagnostic techniques and warnings of possible side effects. The list is curated by a medical advisory committee and is not a “do it yourself” presentation by patients, doctors, or companies. Each listed therapy is linked to a dynamic bibliography, to which patients and clinician/researchers could contribute. including updated searches of PubMed scientific literature citations, data extracted from Patients Like Me, a listing of doctors or institutions recommend the therapy, and any that disagree, along with further reading, and discussion groups relating to that therapy. Patients and doctors in different countries may evaluate the information differently.
Each potential therapy may further be categorized according to the weight of evidence suggesting benefit, harm, or no effect. The following sketch gives a general idea for a graphic interface.

The criteria could be agreed by clinicians and researchers, and they and patients could contribute citations and then therapies could be depicted on the chart. Riluzole is shown as significantly helpful and with very strong evidence. Most therapies will cluster around the origin but a few will start to stand out.
Although the evidence for alternative therapies is weak it is not nonexistent. The PIR helps clinicians as well as patients stay current on the latest PubMed reported studies relevant to a particular therapy.
For example, after a couple of favorable studies about fish oil, there was one showing it accelerates ALS progress in ALS mice. So the new study is worthy of a caveat. The same thing just happened with melatonin. Meanwhile, there are recent reports that raising uric acid by administering inosine may be helpful. So inosine would move upward and to the right on the chart above.
ALS Untangled has developed a set of criteria for its publications about alternative therapies. Likewise, the ALSAT PIR would follow a set of rules developed by consensus and openly presented to users of the Patient Information Resource.
Nonprofit structure with public-private partnerships
The ALSAT PIR is a nonprofit project structured to approach the topic of alternative therapies ethically and in a scientifically rigorous manner. Its mission of promoting health, research, and patient education would qualify the ALSAT PIR for charitable donations. As a nonprofit, the PIR could partner with for profit organizations, in particular, Patients Like Me, to obtain and present private patient data. Public-private partnerships are well-established engines of innovation and improvements in public health. Structuring such partnerships here presents no special problems.
Management
The project is supervised by an advisory board including ALS patients, ALS advocacy group representatives, physicians, and researchers, in particular members of ALS Untangled. The advisory board sets and changes policy, addresses ethical issues, determines staffing, sets rules and criteria for posting alternative therapy entries in the PIR list, and provides input on the types of discussion that should be invited, maintained, or removed from the patient and physician discussion groups.
Modern website tools can keep the site fresh. For example, the literature citations for “melatonin and ALS” could be generated in real time by automatically sending a search query to PubMed. Nonetheless, the PIR requires regular maintenance because new information arises monthly, sometimes weekly, with implications for therapy. Also, discussions need supervision to check the many tendencies toward bias in a variety of directions. These include patients wanting to promote their own anecdotal experience as having more validity than is objectively warranted, doctors being unwilling to accept preliminary evidence as a basis for therapy, in the absence of controlled clinical trial data, inventors of a therapy who may over-promote it, and people with a commercial self-interest in promoting a particular therapy.
A patient-centered approach:
The ALSAT PIR allows ALS patients to establish and drive a very different dynamic between doctors and patients. ALS patients become active participants in defining possible therapies and presenting them to doctors for comment.
With their diagnosis, ALS patients are thrown into a cruel new reality. ALS is terminal and incurable, causing death within 2-5 years for most victims. Some live 10 years or more, and the reasons for their longevity are not well understood. The only drug that has passed a placebo-controlled double-blinded clinical trial is Rilutek (riluzole) for which the data shows, on average, a 2-3 month extension of life.
Some ALS specialists do make recommendations to their patients but their lists are not broadly available for other patients to consider, and they are not published and available for peer review. Many doctors are reluctant to recommend an alternative therapy regimen because it has not been clinically proven. They have an ethical basis for abstaining from recommendations they are not confident about – The Hippocratic oath says to do no harm. But when a patient asks a doctor, “should I take this?” the ethics switch so that the ethical duty becomes: answer the question to the best of the doctor’s ability.
Most ALS patients do more than just take Rilutek. Each patient struggles to find a suitable regimen of diet, supplements, physical therapy, and other drugs with beneficial effects. Many of the options are in the “won’t hurt, might help” category. But some are dangerous, toxic, or may even make the disease progress more quickly. Some are too expensive for an ALS patient to afford. These points were made forcefully at an FDA hearing on February 25, 2013, at which I testified. A summary of the FDA ALS hearing with links to testimony is here. (MDA ALS Newsmagazine, 2/25/2013, “FDA Hearing Highlights ALS Drug Development Concerns”). My written remarks are attached as Appendix 2.
The current system leads patients to self-medicate based on scant or nonexistent scientific data. From the patient’s point of view, this has some benefits and many drawbacks. One benefit is the placebo effect, the phenomenon with many diseases that when patients believe a therapy is having a positive health effect, a sizable percentage of that group actually manifests a health improvement, at least temporarily, as compared to patients who do nothing at all. Indeed, the placebo effect is so well-accepted as clinically significant that the golden standard for all FDA-approved drugs is to show a significant improvement over placebo. The placebo effect is complex, and is factored into clinical trials for ALS drugs. A patient-centered approach may take advantage of the placebo effect.
A related benefit is the feeling of self-control patients maintain by taking action to improve their health. ALS patients routinely report that they will self-medicate, they will take risks, they will try unproven, even dangerous therapies, because the risk of doing nothing is so severe – a steady decline and certain death. So a patient-centered approach gives patients control over the decisions they make to protect their health. This control certainly contributes to mental health, and quality of life.
Generally even the most conservative doctors agree that it is desirable for a patient to continue with a therapy that is in the category of “won’t hurt, might help.” From the patient’s perspective, if it might help the disease, that’s good enough, provided the therapy is not (a) harmful, (b) too expensive, (c) too complex or time-consuming, and that it will not (d) interfere with another therapy, or (e) disqualify the patient from a clinical trial.
Advantages of the ALSAT PIR
Along with ALS Untangled, the PIR can help patients avoid dangerous or costly unproven therapies. It can also direct patients to practical approaches that might help.
Using curated information provided by the Patient Information Resource, ALS patients can improve their own decision-making. By participating in discussion groups, they can help other patients. Doctors can consider what therapies patients are using and contemplating, and thereby modify their own recommendations. Researchers can develop new hypotheses regarding efficacy of given supplements and design experiments to test them, helping shape the research agenda for the disease.
The ALSAT PIR creates a framework where patients may exercise informed choice among current options. By focusing on current therapies, and helping galvanize professional review, this approach would accelerate discovery of new options. When new data becomes available suggesting a common therapy is toxic or dangerous, the PIR can facilitate disseminating the information, thereby reducing risk to patients.
Patient Outcome measures
The new healthcare paradigm requires evaluation of patient outcome measures. The PIR fits into this paradigm, providing ready measures about patient-reported outcomes. Objective evidence about various alternative therapies can be presented along with patient reported evidence regarding e.g. side effects, cost, and impact on disease markers such as the gold standard ALS Functional Rating Scale (ALS-FRS), forced vital capacity (FVC). Patients can be surveyed to understand their decisionmaking process, and in turn this can lead to observations about whether patients are steered away from potentially harmful therapies toward more helpful ones.
Related resources
The ALSAT PIR can work synergistically with many existing sites and information resources. Some of these include the following:
Books
• Richard S. Bedlack, Hiroshi Mitsumoto, Amyotrophic Lateral Sclerosis: A Patient Care Guide for Clinicians (Demos 2012)
• Hiroshi Mitsumoto, Amyotrophic Lateral Sclerosis: A Guide for Patients and Families (Demos 2009)
Patient oriented sites
• Patients Like Me http://www.patientslikeme.com/
• MDA ALS Division http://mda.org/disease/amyotrophic-lateral-sclerosis
• ALS Association http://www.alsa.org/
• Patient and Survivor Family sites
Physician and researcher oriented resources
• ALS Therapeutic Development Institute (ALS TDI)
• ALS Untangled http://www.alsuntangled.com/
• ALS clinics at teaching hospitals (Johns Hopkins Packard Center, Mass General, etc.)
• FDA: ALS hearing http://www.fda.gov/Drugs/NewsEvents/ucm339833.htm
• NIH: National Institute for Neurological Disorders and Stroke (NINDS) http://www.ninds.nih.gov/disorders/amyotrophiclateralsclerosis/ALS.htm
• NIH: National Center for Complementary and Alternative Medicine (NCCAM) http://nccam.nih.gov/health/atoz.htm
• Physical therapists
• Massage therapists
• Pharmaceutical manufacturers
• Supplement manufacturers
• Medical device manufacturers
Suggestions are welcome: mgollin@gmail.com
Appendix 1
ACCELERATING LIFE SAVING ALTERNATIVE THERAPIES:
PATIENT INFORMATION RESOURCE
(ALSAT PIR)
draft August 2013
This list of alternative therapies is based on a variety of sources, including recommendations by ALS doctors and practices of ALS patients. It is intended as a useful source of information for ALS patients, physicians, and researchers. Patients are urged to discuss this list with their doctor in developing an appropriate individualized therapeutic regimen. This list is not intended to be used as medical advice. Click on each therapy listed for more information.
Contact the author for the detailed list.
